Disclaimer: I graduated medical school in 2010. During my education (medical school and residency), I only had a few months in which I operated in a hospital that had no EMR whatsoever. In other words, my experience without an EMR was VERY limited. It was nevertheless quite memorable. This is how I remember it:
Ordering
For typical orders, the following steps were needed.
Step 1: find the physical chart.

Finding the physical chart was one of the most frustrating aspects of inpatient care before computerized physician order entry (CPOE), at least for me. There was a place for the charts in the nursing station, but more often than not, the chart was elsewhere. Usually with the nurse somewhere (sitting outside the room, possibly even in the break room). If the patient went off the floor for a radiology study, the physical chart would go with him.

Step 2: write the order
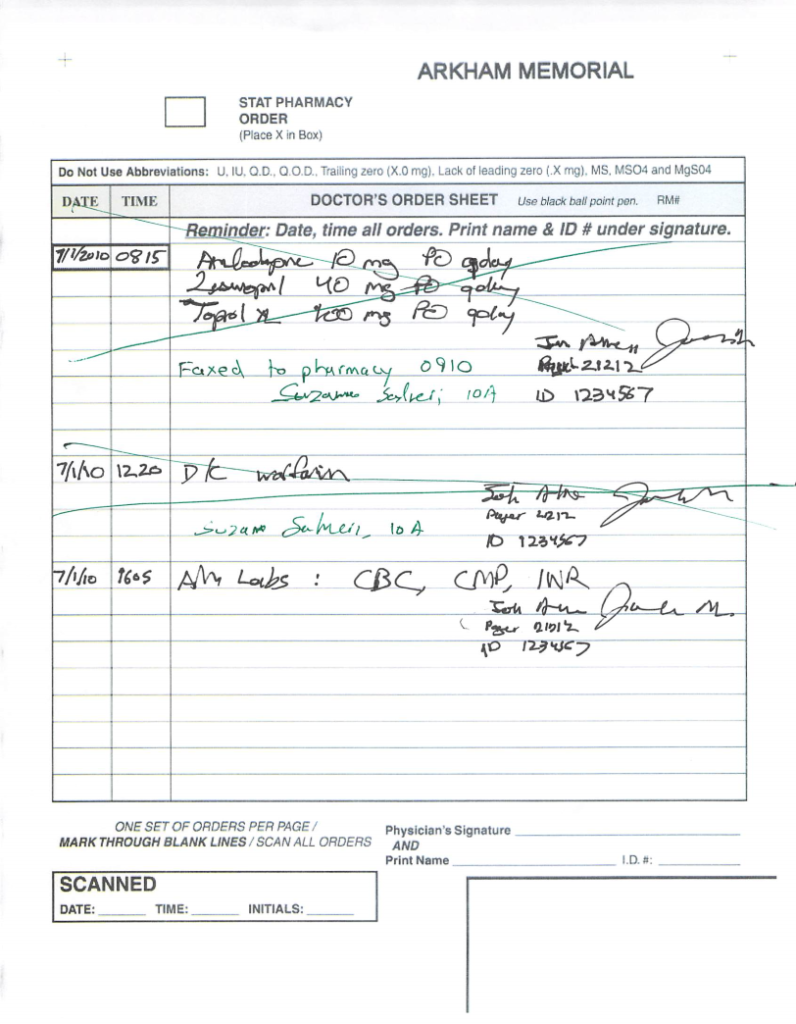
Free-style orders
One would find the order section in the chart, and then go an empty line below the most recently written order. This part of order entry was actually nice–you could just write what you want. Instead of searching for “CBC” and “CMP” and selecting draw times, etc, you could simply write: “AM labs: CBC c diff, CMP”. Of course, this did not always end up with the correct labs being ordered. For example, I quickly learned to write “lactic acid” instead of “lactate”, because “lactate” would always end up being translated to “lactate dehydrogenase”.
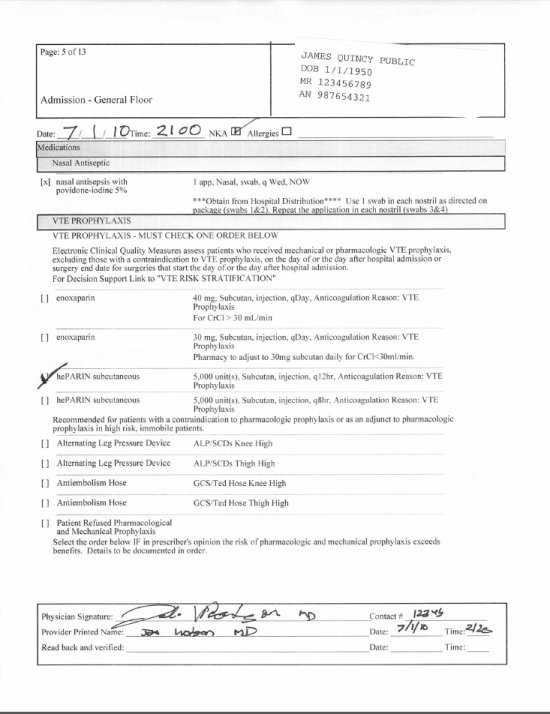
Order set orders
Some orders were part of order sets, which were pre-printed sheets of paper with multiple orders written on them. One would simply put a check by which order he/she wanted. These were common for admissions. Some of the more complicated orders (e.g. argatroban infusion) had them as well. These were probably easier to do than the CPOE equivalent (assuming one could actually find the order set sheets).
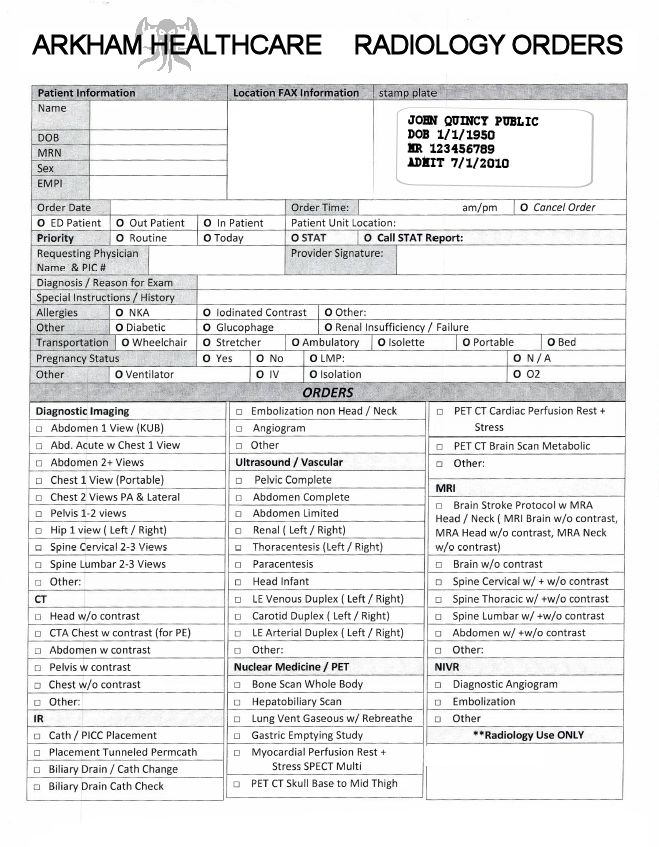
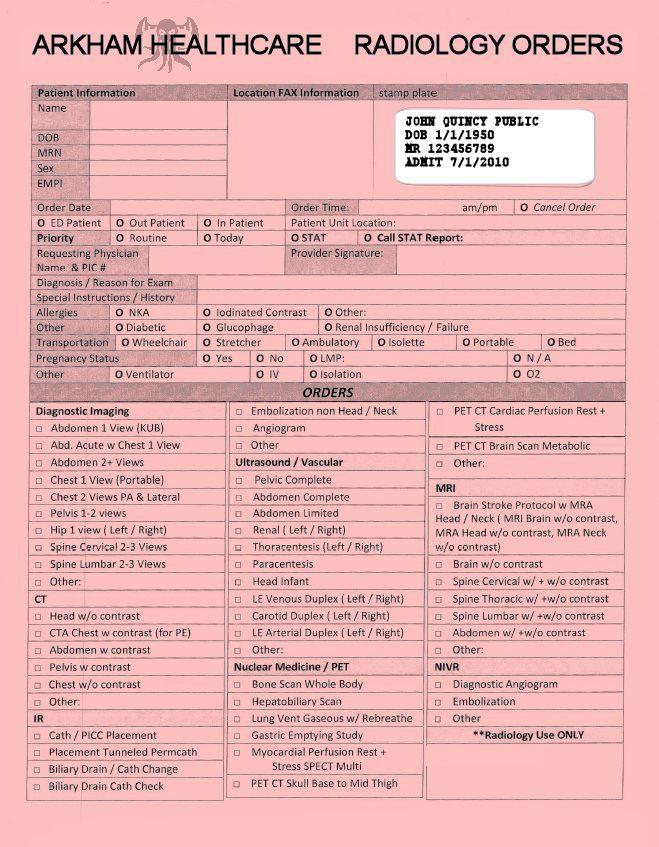
Radiology orders
Radiology orders were also on a pre-printed paper form, but they were carbon-copy style (three-ply). You had to affix a patient label on every sheet. And then you checked which box you wanted.
Step 3: give chart to unit clerk
One would open the 3 ring binder, and shift the active order sheet up so that it juts out from the top of the binder. And place the binder in the stack of “Incoming Order Charts” next to the unit clerk.
The unit clerk had the job of going through all the orders and doing different things to them depending on what type of order it was. He/she would fax the medication orders to the pharmacy. For the lab orders, I seem to remember the clerk having to enter those orders into a custom piece of lab software.
After orders were processed by the unit clerk, he/she would sign or stamp below them, and then cross out the text to signify that the order had been processed.
Clinical notes
Writing notes was probably easier in the pre-EMR era (as it is easy to scribble), but reading notes was significantly harder (as it is hard to read scribbles).
To write an H&P, one would often use a template–these were pre-printed forms that had all the necessary blank spaces (and sometimes check boxes for the Review Of Systems). Progress notes were typically written on the standard lined (but otherwise blank) paper in the chart. Discharge summaries were the formal note of the bunch, and thus would typically be dictated.
To read notes, one would need to find the chart (see above) and flip to the most recent entry. In my experience (or at least by my recollection), any note written by anyone other than me was incredibly hard to read. For some reason, providers tended to write in cursive. I remember coming across a word that was totally indecipherable but yet very important to the patient’s diagnosis. I showed the chart to about 10 other MDs/RNs; none of them could guess what that word was.
Radiology
In the days before PACS, one had to view x-rays on x-ray film, which was a large floppy sheet of plastic. To view the image on the film, one had to place it on a light box on the wall–this provided back lighting needed to properly view the image.

CT scans and MRIs also had a films–these had tiny images of each slice on a grid. I’m not sure if the radiologists were using these films or using a computerized system to interpret the scans, but the films are what we had. (If anyone knows more about the CT/MRI physical films, please comment/email).